For staff working across GP practices, community clinics, child health services and immunisation teams
Why the change?
➤ On 31 October 2025, UK Health Security Agency (UKHSA) and NHS England announced that from 1 January 2026 a new routine childhood vaccination programme will include the combined vaccine for measles, mumps, rubella and varicella (chickenpox): the so-called MMRV vaccine. (GOV.UK)
➤ The move comes after recommendation by the Joint Committee on Vaccination and Immunisation (JCVI) to introduce varicella into the routine childhood immunisation schedule, via the combined MMRV preparation. (GOV.UK)
➤ Until now, the routine UK schedule used the MMR vaccine (measles, mumps and rubella) and varicella vaccine was not offered universally to all children. (meningitis.org)
➤ For healthcare staff, this means an important update to practice workflows, vaccine ordering, scheduling and communicating with parents/carers.
What are the key changes?
Here are the changes that staff need to be aware of:
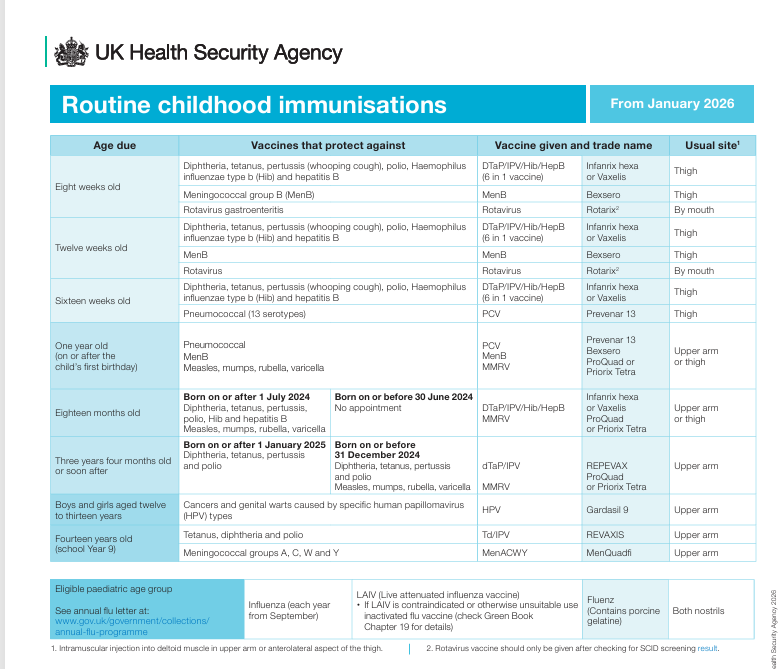
• New routine schedule from 1 Jan 2026
From that date, children eligible will be offered the MMRV vaccine instead of the MMR (for the main schedule) for certain cohorts. (GOV.UK)
The eligibility depends on date of birth.
For example:
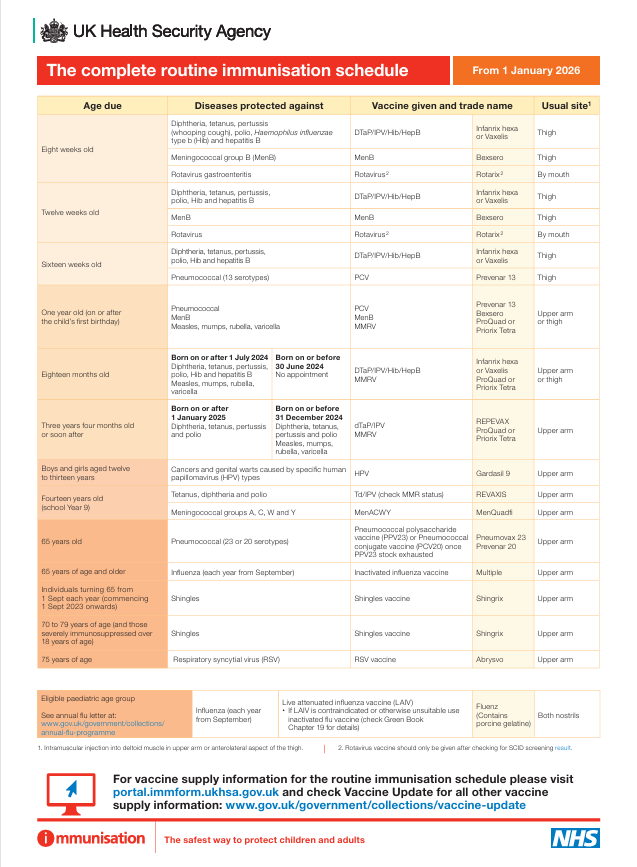
- Children born 1 Jan 2025 or later: two doses of MMRV — first at 12 months, second at 18 months. (GOV.UK)
- Children born 1 July 2024 to 31 Dec 2024: first dose MMR at 12 months, then MMRV at 18 months, then MMRV at 3 yrs 4 months. (GOV.UK)
- Children born 1 Sept 2022 to 30 June 2024: one dose of MMRV at 3 yrs 4 months (instead of MMR) if they have already had the 12-month MMR. (GOV.UK)
• Selective catch-up programme
A one-dose MMRV catch-up will be offered 1 November 2026 to 31 March 2028 to children aged 3 yrs 4 months to under 6 yrs (born 1 Jan 2020 to 31 Aug 2022) who have no history of chickenpox infection or two doses of varicella vaccine. (GOV.UK)
• MMR vaccine (without varicella) will cease in routine programme
After 1 Jan 2026, MMR (without varicella) will no longer be used in the routine childhood programme (for those cohorts now eligible for MMRV).
MMR will still be available outside the routine programme (e.g., older individuals who missed their doses). (GOV.UK)
• Operational and antenatal implications
- Practices will need to update call/recall systems, immunisation schedules, and check eligibility by date of birth.
- Vaccine ordering: new vaccine stock (MMRV) will be required; guidance suggests practices should hold no more than two weeks’ worth of MMRV stock and rotate fridge stock to minimise wastage. (Nursing in Practice)
- Staff must be supported with training and communications tools to implement the change effectively. (GOV.UK)
Why it matters: for children, families and services
- Chickenpox (varicella) is usually mild, but complications can occur (especially in immunocompromised children, infants, and pregnant women). Including varicella in the routine schedule means the population will gain a wider protective benefit.
- Using a combined vaccine (MMRV) reduces the number of injections and simplifies the schedule (one combined product rather than separate MMR + varicella).
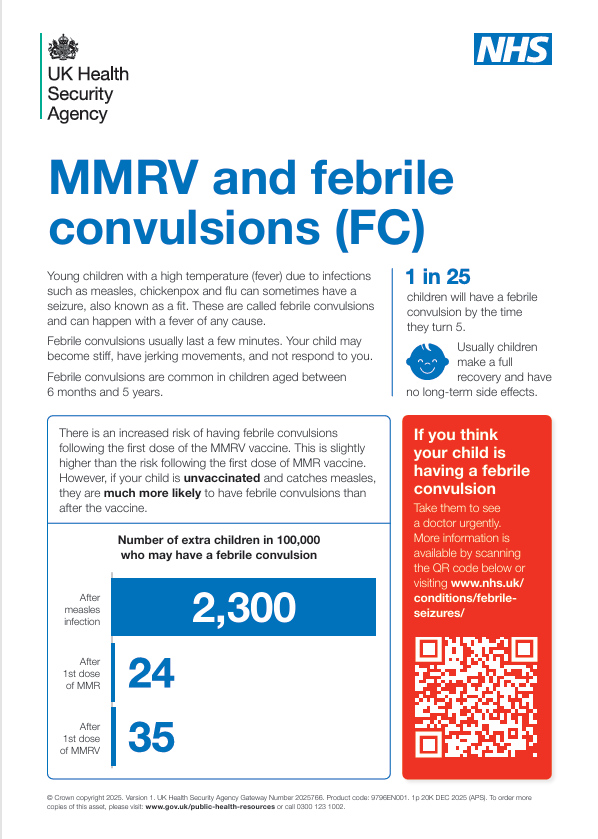
- Earlier second dose (18 months instead of 3 yrs 4 months for some cohorts) means children are fully protected earlier—important given outbreaks of measles in recent years and modest uptake levels. (vaccineknowledge.ox.ac.uk)
- For staff, this change presents an opportunity to reinforce vaccine uptake messaging, tackle any vaccine hesitancy proactively, and support catch-up efforts for children who may have missed previous doses.
Key actions for healthcare staff
Here’s a practical checklist for you and your team to prepare and implement the changes:
- Update your practice/system protocols
- Ensure the immunisation schedule and system flags reflect the new eligibility criteria by date of birth.
- Review call/recall lists for children due at the new 18-month appointment.
- Brief admin/reception teams about the change so appointments are booked correctly.
- Stock and logistics
- Order the MMRV vaccine in time; check whichever brand your region will supply (e.g., Priorix-Tetra or ProQuad). (Nursing in Practice)
- Monitor stock rotation and wastage: hold no more than two weeks of stock and ensure fridges are compliant.
- Update cold-chain logs, accountability sheets to include MMRV.
- Training and communication
- Ensure clinical staff (nurses, GPs, health visitors) are aware of the new schedule, eligibility criteria, catch-up programme.
- Prepare brief information for parents/carers explaining the change: why varicella is included, what the combined vaccine means, when the child will be invited.
- Be ready to answer questions about safety, side-effects, and use phrases that normalise the change (“From January we will offer the combined MMRV…”) rather than emphasising “change”.
- Catch-up programme awareness
- From 1 Nov 2026—31 Mar 2028, ensure children aged 3 yrs 4 months to under 6 yrs (DOB 1 Jan 2020-31 Aug 2022) who are missing varicella protection are offered the one-dose MMRV catch-up.
- No need to check chickenpox history before offering the vaccine. (Nursing in Practice)
- Audit and monitor uptake
- Keep track of numbers of children offered MMRV, number who received it, and follow-up for those who did not attend.
- Identify children who may still be on old schedule and ensure they are transitioned appropriately.
- Be prepared for queries
- Parents may ask: Why add chickenpox vaccine now? Will it increase side effects? What about children who had chickenpox already?
- Explain that including varicella strengthens protection and aligns with national recommendations.
- For children who already had chickenpox, the programme guidance states that there is no requirement to check disease history — the vaccine may still be offered. (GOV.UK)
- Side-effect profiles remain acceptable in the UK context; combined MMRV vaccines have been used safely elsewhere. (vaccineknowledge.ox.ac.uk)
- Parents may ask: Why add chickenpox vaccine now? Will it increase side effects? What about children who had chickenpox already?
FAQs (for practice teams)
Q: What if a child has already had two doses of MMR before 1 January 2026?
A: They would have received full protection against measles, mumps and rubella under the previous schedule. For varicella protection: check eligibility for catch-up (if aged 3 yrs 4 months-under 6 yrs by 31 Dec 2025 and no chickenpox/vaccine history) and offer one dose of MMRV between Nov 2026–Mar 2028.
Q: Can the MMRV vaccine be given to children who already had chickenpox?
A: Yes — the guidance states there is no requirement to check for past chickenpox infection before offering the catch-up dose. (Nursing in Practice)
Q: What about children born before 1 January 2025 but after 31 August 2022 (i.e., 18 months to under 3 yrs 4 months on 31 Dec 2025)?
A: These are eligible for one dose of MMRV at their 3 yrs 4 months appointment (instead of MMR) providing they have already received the first MMR at 12 months. (GOV.UK)
Q: Is the MMRV vaccine interchangeable with MMR?
A: Yes — the two licensed MMRV vaccines are considered clinically equivalent and interchangeable. (Nursing in Practice)
Final thoughts for health-care teams
This programme change represents a significant step in strengthening childhood immunisation in England (and the UK) — adding varicella to the routine schedule via the combined MMRV vaccine offers broader protection and aligns with international practice. For healthcare staff, the success of the roll-out will rest not only on correct logistics and stock management, but on clear communication with families, vigilance in call/recall systems, and proactive outreach to ensure no eligible child is missed.
By preparing now — updating systems, briefing teams, and planning for both routine and catch-up pathways — your practice or service can ensure a smooth transition when 1 January 2026 arrives.
Thank you for all you do in delivering childhood immunisations. Your role is vital in safeguarding children’s health and supporting population protection.
Useful resources:
MMRV Vaccination programme
New UK routine childhood schedule from January 2026
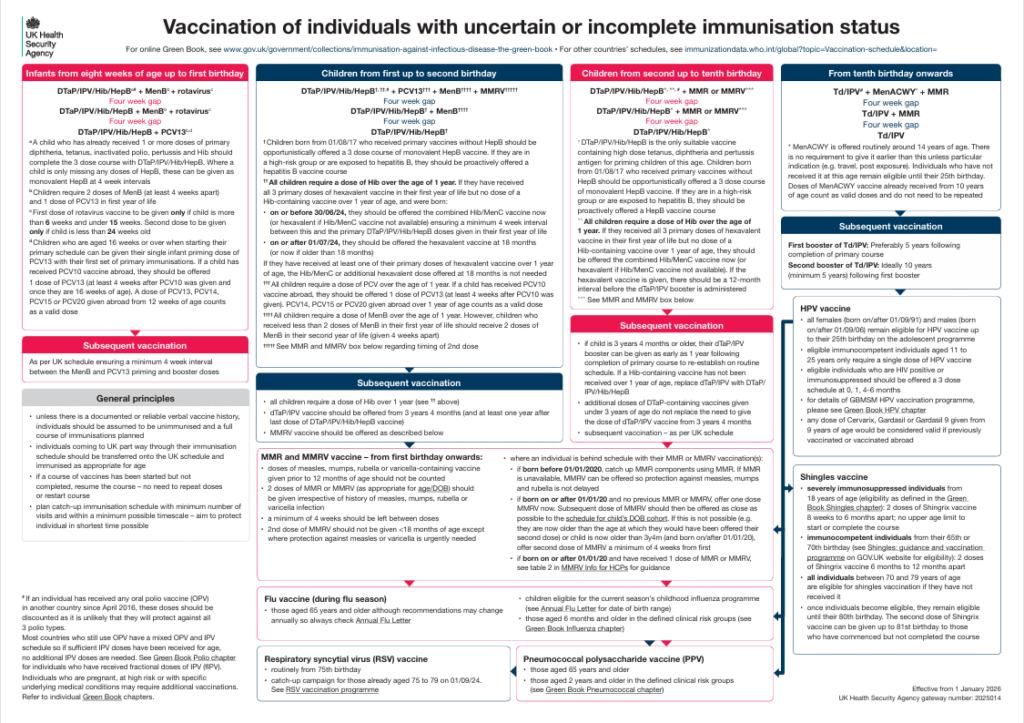
Uncertain/Incomplete Vaccine history/status
Information for Healthcare professionals:
MMRV vaccination: information for healthcare professionals – GOV.UK
This guidance for healthcare professionals describes eligibility, administration and safety, and answers frequently asked questions about the new vaccination programme.
Eligibility Tables:
MMRV leaflet
Measles Green Book Chapter updated:
Varicella Green Book Chapter updated: