Bite‑size clinician FAQ for parent and student consultations
Meningococcal group B (MenB) remains the leading cause of invasive meningococcal disease (IMD) in England, responsible for over 80% of cases (313 of 378) in 2024/25. While overall incidence is low, the disease is severe and can progress rapidly. Recent high-profile incidents, such as the Kent cluster, have triggered significant public concern, driving increased demand for vaccination, reassurance, and clinical advice across primary care and community services.
Here is the information and later scripted suggestion of how to manage the FAQs of worried parents/students/general public.
Epidemiology and “how worried should I be?”
- Q: How common is MenB in the UK right now?
A: In England 2024/25 there were 313 MenB cases (82.6% of all IMD), out of 378 total IMD cases. [GOV.UK] - Q: Who gets MenB most often?
A: It is most common in babies/young children and there is a second peak in teenagers/young adults; in 2024/25 most IMD under 25 was MenB. [GOV.UK] - Q: Is MenB “rare but serious”?
A: Yes. IMD incidence in England is reported as below 1 per 100,000, but progression can be rapid and fatalities occur (England IMD CFR 8.2% in 2024/25). GOV.UK]
Transmission, carriage, incubation and speed of illness
- Q: How does MenB spread?
A: Mainly via close/prolonged contact with someone carrying meningococci in the nose/throat (often without symptoms); outbreaks sometimes occur in shared living settings (e.g., university halls). [UKHSA] - Q: What is the incubation period?
A: UK guidance describes incubation usually 3–5 days, and UK immunisation programme materials cite 2–7 days. [GOV.UK] - Q: How quickly can people deteriorate?
A: UKHSA messaging emphasises that bacterial meningitis/septicaemia can make someone seriously unwell within hours, so repeated checking and clear safety‑netting are essential. [UKHSA]
Signs and symptoms by age (include “don’t wait for rash”)
- Q: What should I tell everyone to watch for?
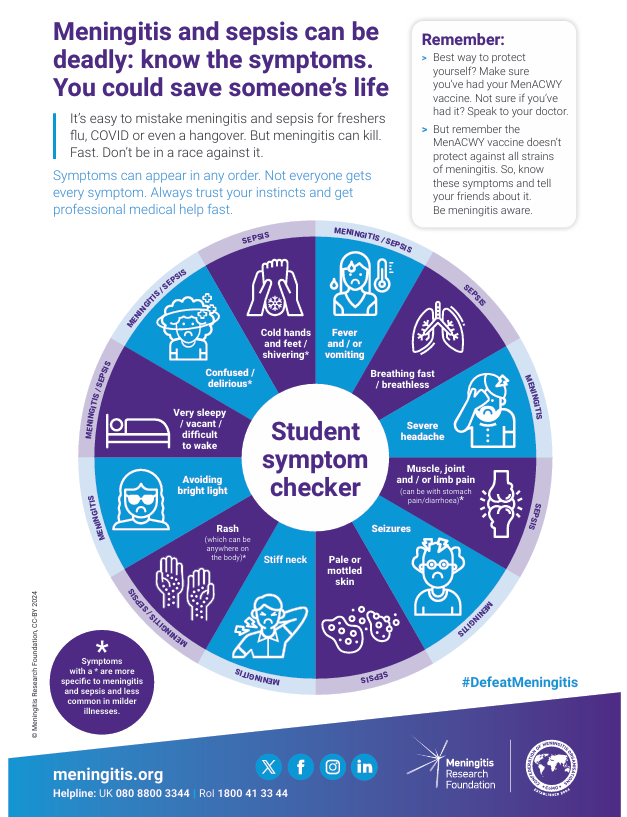
A: Fever, vomiting, severe headache, cold hands/feet, confusion, rapid breathing, severe limb/joint pains, and any non‑blanching rash; symptoms may appear in any order and some may be absent. [UKHSA] - Q: Infant‑specific features (babies): what is different?
A: Poor feeding/refusing feeds, drowsy or difficult to wake, floppy or stiff/jerky movements, irritable when picked up, high‑pitched cry, grunting, abnormal breathing patterns, pale/blotchy/blue skin, and a non‑blanching rash may occur. [UKHSA] - Q: Child features (toddlers/children): what do charities emphasise early?
A: Limb pain, pale skin and cold hands/feet can appear earlier than classical meningitis signs (neck stiffness/photophobia) and before rash. [MENINGITIS.ORG] - Q: Teenagers/students: what gets missed?
A: Early symptoms can look like flu or hangover; NICE flags that altered behaviour in young adults may be wrongly attributed to alcohol/substances, delaying care. [UKHSA]
Red flags and immediate actions
- Q: What are NICE “red flags” for meningococcal disease?
A: Purpura (non‑blanching lesions >2 mm), rapidly progressive/spreading non‑blanching petechial/purpuric rash, or meningitis symptoms combined with a non‑blanching rash. [NICE] - Q: Can I rule out meningococcal disease if there is no rash?
A: No. NICE explicitly says not to rule it out just because there is no rash. [NICE] - Q: What should clinicians advise if meningitis/septicaemia is suspected?
A: Emergency transfer (999/A&E) and do not delay for rash or to “see how they go”; UKHSA messaging advises calling 999 or going to A&E if concerned about meningitis/sepsis. [UKHSA] - Q: Pre‑hospital antibiotics—when and what?
A: NICE: do not delay transfer to give antibiotics; if transfer will be significantly delayed and meningococcal disease is strongly suspected, give IM/IV ceftriaxone or benzylpenicillin outside hospital (unless severe allergy). [NICE]
Differential diagnosis “cues” in worried‑well settings
- Q: What common presentations can look similar early?
A: Early symptoms can resemble viral URTI/flu, gastroenteritis, migraine, or “freshers’ flu”/hangover; time‑course (rapid worsening), systemic toxicity, cold extremities/limb pain, and rash evolution help differentiate. [UKHSA] - Q: What is a safe one‑liner to avoid false reassurance?
A: “Most fevers are not meningococcal disease, but meningococcal disease can worsen fast, if they get rapidly more unwell or develop a non‑blanching rash, seek emergency care immediately.” [UKHSA]
Antibiotic chemoprophylaxis after a case: who, when, what
- Q: Who counts as a “close contact”? (UK definition used by public‑health teams)
A: Prolonged close contact in a household‑type setting during the 7 days before onset, including people living/sleeping in the same household, pupils in the same dormitory, partners, or university students sharing a kitchen in halls. [GOV.UK] - Q: Who is usually not a close contact (so doesn’t routinely need antibiotics)?
A: Same school/class/tutor group, work colleagues, friends, attending the same event, and low‑level salivary contact such as brief kissing or sharing drinks/vapes are listed as not meeting the definition (public‑health judgement may apply in borderline scenarios). [GOV.UK] - Q: How quickly should prophylaxis be given?
A: As soon as possible. UK guidance says ideally within 24 hours after IMD is suspected/confirmed; if notification is delayed, prophylaxis may still be offered up to 28 days after onset (risk beyond this is low). [GOV.UK] - Q: First‑line agent and doses?
A: UK guidance recommends single‑dose ciprofloxacin (including in pregnancy), with age‑banded dosing: ≥12y 500 mg; 5–11y 250 mg; 1–4y 125 mg; <1y 30 mg/kg (max 125 mg; off‑label). [GOV.UK] - Q: If ciprofloxacin is unsuitable?
A: Rifampicin is an alternative; ceftriaxone requires injection; choice may be influenced by resistance risk (e.g., travel‑associated resistance) and interactions (rifampicin reduces hormonal contraceptive effectiveness). [GOV.UK] - Q: Pregnancy and prophylaxis, what should I say?
A: UK guidance: chemoprophylaxis options in pregnancy include ciprofloxacin, ceftriaxone or azithromycin; UK guidance also states ciprofloxacin is recommended for use in pregnancy. [GOV.UK] - Q: Does the index case need eradication prophylaxis?
A: If treated with IM/IV cephalosporins (e.g., ceftriaxone/cefotaxime) they do not need prophylaxis; if treated with other antibiotics, offer chemoprophylaxis when able to take oral medication, ideally before discharge. [GOV.UK] - Q: Should close contacts be offered MenB vaccine after a single sporadic MenB case?
A: UKHSA public‑health guidance: after a single confirmed/probable serogroup B case, MenB vaccination is not recommended for close contacts, even if strain is predicted vaccine‑preventable (exceptions relate to clinical risk groups immunisation status, and outbreak/cluster management). [GOV.UK]
Vaccination: schedules, catch‑up, effectiveness, safety and student guidance
- Q: What is the routine infant MenB schedule now?
A: From 1 July 2025: 8 weeks, 12 weeks, and 1 year (2+1 schedule). [GOV.UK] - Q: What about catch‑up if a baby missed doses?
A: Missed MenB doses can be given free up to the second birthday; UK guidance provides age‑appropriate catch‑up schedules (e.g., <12 months: 2 doses ≥4 weeks apart plus booster at 12 months). [GOV./UK] - Q: What should I say about effectiveness?
A: UK programme materials state the infant programme reduced disease in vaccinated cohorts by around 75% compared with unvaccinated trends; observational UK analyses estimate high vaccine effectiveness in fully immunised children. [GOV.UK] - Q: Does MenB vaccine stop carriage/spread (herd immunity)?
A: UK programme guidance states it is effective against MenB IMD in vaccinated individuals but does not protect against carriage, so is not expected to generate broad herd protection. [GOV.UK] - Q: Does the MenB vaccine cover all MenB strains?
A: No. Green Book estimates ~66–88% strain coverage in England/Wales; UKHSA public‑health guidance similarly notes incomplete strain coverage (and emphasises ongoing symptom vigilance even after vaccination). [GOV.UK] - Q: Safety: what are the typical side‑effects clinicians should pre‑empt?
A: Fever and local reactions are common, especially when co‑administered with routine infant vaccines; product information lists fever/irritability and injection‑site tenderness/erythema as very common in infants, and headache/malaise/injection‑site pain as very common in adolescents/adults. [EMC] - Q: Paracetamol: what is the UK advice with infant MenB?
A: UK advice recommends prophylactic paracetamol after MenB doses at 8 and 12 weeks (three doses, spaced 4–6 hours apart), because fever is more common with co‑administration; guidance notes this is specific to post‑vaccination fever management and aims to avoid delaying care for unexplained fever at other times. [NHS] - Q: Contraindications/precautions?
A: Do not give after confirmed anaphylaxis to a previous dose/ingredient; defer during severe febrile illness; pregnancy data are limited (SmPC: insufficient clinical pregnancy data, but vaccination should not be withheld when exposure risk is clear). [EMC] - Q: Students: “Am I protected by MenACWY?”
A: No. MenACWY protects against A, C, W, Y, not MenB; UK sources emphasise MenACWY remains important for new university entrants (eligible up to age 25), but does not cover MenB. [GOV.UK] - Q: Students: “Can I get MenB on the NHS?”
A: Routine MenB is for infants; UKHSA states those born before 1 May 2015 did not receive MenB as part of the schedule and there is no routine NHS catch‑up unless in a clinical risk group, though outbreak responses may include targeted vaccination. [UKHSA]
Outbreak definitions and response (what to tell parents/students about “why some people get antibiotics/vaccine”)
- Q: What is a “cluster” vs “outbreak” in UKHSA terms?
A: Cluster = ≥2 confirmed/probable IMD cases linked by time/place not yet shown to be different strains; outbreak = cluster with cases epidemiologically linked and caused by the same strain. [UKHSA] - Q: What happens operationally after a suspected case?
A: Public‑health management focuses on urgent case notification, contact tracing, rapid chemoprophylaxis for close contacts, and targeted vaccination only in defined cluster/outbreak scenarios after assessment of serogroup/strain and risk group boundaries. [UKHSA] - Q: Why does public health keep emphasising antibiotics (not immediate mass vaccination)?
A: Chemoprophylaxis aims to eradicate carriage in the close‑contact group and reduce secondary cases; UKHSA cites up to 89% reduction in household secondary‑case risk and stresses speed (ideally within 24 hours). (UKHSA) - Q: Pregnancy and outbreak vaccination, any special note?
A: UKHSA guidance notes MenB vaccination is not advised for pregnant close contacts in an outbreak setting due to limited data and reactogenicity (pyrexia), recommending specialist advice for high‑risk pregnant individuals (e.g., complement‑inhibitor therapy). [UKHSA]
Clinician scripts – suggested responses to FAQs
- Parents (child ill, no clear red flags yet):
“Most fevers are not meningitis, but meningococcal disease can worsen in hours. If they become rapidly more unwell, hard to wake, have cold hands/feet, severe limb pain, breathing fast, or develop a rash that doesn’t fade under pressure, seek emergency help, don’t wait for a rash.” [UKHSA] - Students (worried after a case in halls/university):
“Public health defines who needs preventive antibiotics based on close contact, typically household‑type exposure like sharing a kitchen in halls. If you’ve been contacted, take the antibiotics as soon as possible. If you feel rapidly worse or develop a non‑blanching rash, call 999.” [UKHSA] - “Why not antibiotics for everyone in the class/lecture?”
“After a single case, risk outside the close‑contact group is low; antibiotics are targeted to those with household‑type exposure or heavy droplet exposures, to avoid unnecessary antibiotics and focus on those most likely to benefit.” [UKHSA]
References:
What is meningitis? Symptoms, risks and how to protect yourself – UK Health Security Agency

Guidance for public health management of meningococcal disease in the UK
Meningitis Research Foundation | The world’s leading meningitis charity
Cases of invasive meningococcal disease notified in Kent – GOV.UK
Student-Symptom-Poster-MRF-2024-2.pdf
Private Men B vaccines available at Vaccination Centre – 44 Derngate call 01604 439270
Need more information – join one of our Annual Immunisation Updates – Training dates 2026 – Immunisation & Vaccination Courses